
Vesicoureteral Reflux (VUR) correction in children
At a Glance:
1. What is vesicoureteral reflux or urinary reflux in children?
2. What are the causes of vesicoureteral reflux?
3. What are the symptoms of vesicoureteral reflux?
4. What is the grading of vesicoureteral reflux?
5. How do doctors diagnose vesicoureteral reflux?
6. What is the treatment of vesicoureteral reflux?
7. What lifestyle and home remedies can parents of children with VUR follow?
8. How should one choose a facility for the treatment of vesicoureteral reflux?
What is vesicoureteral reflux or urinary reflux in children?
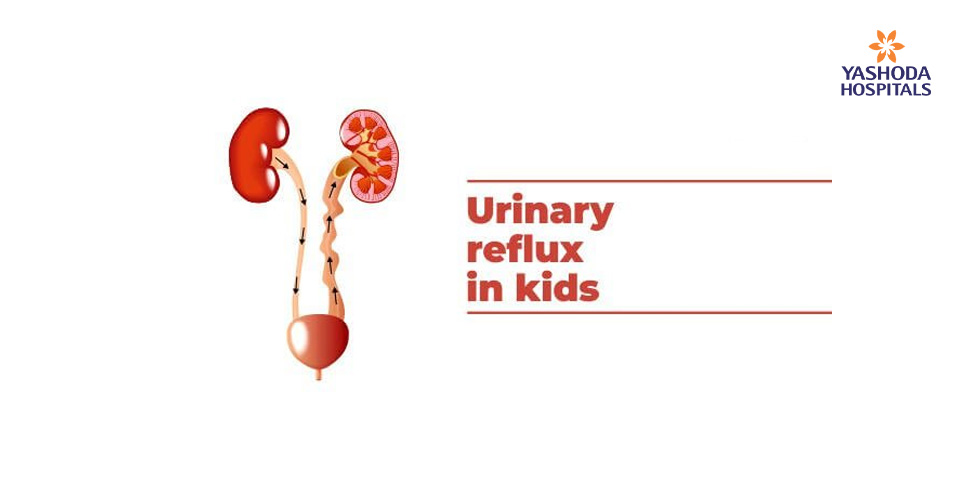
Vesicoureteral reflux (VUR) is a medical disorder of the urinary system. The urinary system is composed of the kidneys, ureters, bladder, and urethra that together excrete waste products from the body via urine. Thin tubes called the ureters to carry urine from the kidneys down to the bladder. The urine is stored in the bladder before it exits the body through another tube called the urethra during urination.
In the normal state, the flow of urine is unidirectional, from the kidneys to the urethra, through the ureters. However, in VUR the direction of this flow gets reversed and the urine flows back into the ureters and kidneys from the urethra.
Vesicoureteral reflux is diagnosed more often in infants and children up to 2 years of age. Girls have a much higher risk of having this condition than boys.
The risk of developing recurrent kidney infections increases in children with VUR. Over some time, recurrent infections can lead to damage and scarring of the kidneys.
Children with VUR are managed by pediatric nephrologists who treat children with problems of kidney or pediatric urologists who perform surgeries of the genital and urinary tract of children.
What are the causes of vesicoureteral reflux?
Vesicoureteral reflux can take two forms namely, primary and secondary:
Primary vesicoureteral reflux: A defect in the valve that prevents the backflow of urine from the bladder into the ureters may be present since birth in the primary vesicoureteral reflux. It is the more common type.
With the lengthening and straightening of the ureters, as the child grows, the function of the valve may improve. Consequently, the reflux gets corrected.
The exact cause of the defect remains unknown. However, it is suspected to be genetic, as it tends to run in families. This defect is more common in boys.
Secondary vesicoureteral reflux: A blockage or defect of the bladder muscle or damage to the nerves that control normal bladder emptying, may lead to failure of the bladder to empty properly.
What are the symptoms of vesicoureteral reflux?
Though each child may have some variability in the symptoms, some of the common signs and symptoms of vesicoureteral reflux may include:
- Urinary tract infection: Children, especially boys below 5 years of age are unlikely to get urinary tract infections (UTI). If a child shows symptoms of UTI, he/she is highly likely to have VUR as the underlying cause of UTI. The signs and symptoms of UTI can include:
- Frequent urgency to pass urine
- Burning sensation while passing urine
- Cloudy urine
- Fever
- Pain in the flank or abdomen
In the case of infants with vesicoureteral reflux UTI may have the following symptoms:
- Unexplained fever
- Lack of appetite
- Irritability
- VUR may cause inflammation or swelling of the kidney that can be observed as an abdominal mass
- Children with chronic VUR may have poor weight gain
- Long-standing damage to the kidneys and the resultant buildup of wastes can lead to high blood pressure.
As the symptoms of VUR can resemble other conditions or medical problems, it is always recommended that a pediatrician be consulted for an accurate diagnosis and further management of the condition.
What is the grading of vesicoureteral reflux?
The severity of VUR can occur in varying degrees, ranging from very mild to severe. The urine may back up only up to a short distance in the ureters in the milder form, whereas it can cause kidney infections and permanent damage to the kidneys in the severe form.
The pediatrician or pediatric urologist may assign a grade ranging from 1-5 with the diagnosis of the condition. The grade indicates the degree of reflux. The higher the grade, the more severe is the reflux.
How do doctors diagnose vesicoureteral reflux?
VUR may sometimes be initially suspected before a child is born. If the prenatal ultrasound (a check-up during) shows hydronephrosis or stretching of the kidney of the fetus, it may indicate that reflux may be present.
The pediatrician or pediatric urologists usually diagnose VUR based on a detailed medical history, physical examination, and investigations. The diagnostic tests for VUR include:
Voiding cystourethrogram (VCUG): It is an X-ray test to evaluate the urinary tract. A small hollow tube or a catheter is placed in the urethra. Once the catheter is in place, the bladder is filled with a liquid dye. As the bladder fills and empties, a series of X-ray images are taken. Any reverse flow of urine into the ureters and kidneys can be observed in the X-rays as the dye appears white in these images.
Renal ultrasound: The size and shape of the kidney can be assessed with a renal ultrasound. The presence of any abnormality like a mass, cyst or a stone, or presence of any obstruction can be identified using a renal ultrasound. The stretching or scarring of the kidneys due to reflux can also be visualized with a renal ultrasound.
Blood tests: Kidney function may be measured with different blood tests.
A urine culture may be needed to confirm a UTI.
What is the treatment of vesicoureteral reflux?
Treatment for VUR depends on many factors like:
- Age of the child, health status, and medical history
- Grade of VUR
- Fitness for surgery or therapies
- Personal needs and preferences
VUR Grade 1-3: In most cases of grade 1-3 VUR, active treatment may not be required. Generally, over some time, the reflux may resolve on its own. This usually happens within five years.
Preventive antibiotic therapy is recommended by the Indian Society of Pediatric Nephrology for children with VUR to prevent any infection from moving to the kidneys. Preventive antibiotics are generally prescribed at a lower dose than that for treating an infection. Such children should also undergo periodic urine tests.
Periodic physical exams and urine tests help in early detection of breakthrough infections
Occasional radiographic scans of the bladder and kidneys help to assess if the child has outgrown vesicoureteral reflux.
Surgical treatment is advised only in rare cases of grade 1-3 VUR.
VUR Grade 4-5: Children with grade 4 and 5 VUR may require surgery to repair the defect in the valve between the bladder and each affected ureter. A flap-valve apparatus is created during the procedure by the surgeon. The apparatus prevents the urine from flowing into the kidney. The scarred kidney and ureter may need to be surgically removed in the more severe cases.
The common methods of surgical repair include:
- Open surgery: It isperformed using general anesthesia, a lower abdominal incision known as bikini incision, is made to repair the condition. The most common type of surgery is ureteral reimplantation. Reflux is prevented by opening the bladder and repairing the ureters. Open surgery has a high success rate of 95 – 97 percent.
The VUR may persist in a few children even after the surgery. However, it generally resolves on its own without much intervention.
A few days of stay may be required in the hospital after the surgery. A catheter is kept in place to drain the child’s bladder during recovery in the hospital.
- Robotic-assisted laparoscopic surgery: With the same objective as open surgery to repair the valve between the ureter and the bladder, this technically advanced surgery is performed using very small incisions.
The main advantage of this procedure is the smaller incisions and fewer chances of bladder spasms as compared to open surgery. Though the operating time may be longer, the postoperative recovery time is reduced.
- Endoscopic surgery: This is a minimally invasive procedure as compared to open surgery. The procedure is performed under general anesthesia, as outpatient surgery. A cystoscope, that is a thin tube fitted with a camera is inserted through the urethra. The camera helps the pediatric urologist to visualize inside the child’s bladder. A bulking agent is injected around the opening of the affected ureter. The valve’s ability to close properly gets strengthened due to the agent.
What lifestyle and home remedies can parents of children with VUR follow?
The most common complication of vesicoureteral reflux is urinary tract infections and it can be painful. The discomfort of the child suffering from UTI can be managed to a certain extent until antibiotics clear the infection by following some remedies like:
- Hydration: The child suffering from VUR should be encouraged to drink adequate fluids,particularly water. The urine gets diluted with sufficient water. This also may help in flushing out bacteria.
- Warm-up: A heating pad, blanket or towel can be used to minimize the feeling of pressure or pain with warmth. The towel or blanket should be just warm and placed over the child’s abdomen.
Bowel dysfunction (BBD) in certain children may cause VUR. Healthy toileting habits should be encouraged in such children by preventing constipation with a nourishing diet. Bladder emptying every few hours while the child is awake should be encouraged too.
How should one choose a facility for the treatment of vesicoureteral reflux?
All cases of VUR aren’t the same. Consequently, the treatment of vesicoureteral reflux should follow an individualized approach to medical care. Care should be sought ideally at a high volume specialized center with pediatric urologists/pediatricians having ample expertise and experience in managing such conditions. Emphasis should be laid on a thorough medical history and examination to fit each child and family.
VUR due to conditions like bowel and bladder dysfunction with recurrent UTI can cause a significant impact on the body’s physiology, a center with multidisciplinary services and state-of-the-art services like pelvic floor rehabilitation and biofeedback program for holistic care is ideal for the treatment of VUR.
Conclusion:
Even though many children overcome the VUR by age 5, it is imperative that VUR if present should be diagnosed early and closely monitored with the child’s pediatrician. Getting treatment if the need is, will help prevent any lasting damage to the child’s kidneys and bladder.
When surgery for VUR is necessary, the pediatric care team at Center for Paediatrics, Yashoda Hospital implements a surgical plan that is customized as per individual needs to give the best results with the least invasive method. The pediatric specialists at Yashoda hospital have a vast experience in almost all the sub-disciplines of pediatric medicine and surgery. The hospital offers state-of-the-art pediatric care in the form of open communication, emotional support and education to all patients and their families on the management of medical problems like VUR.
Reference:
- Mayo Clinic. Vesicoureteral reflux. Available at. https://www.mayoclinic.org/diseases-conditions/vesicoureteral-reflux/symptoms-causes/syc-20378819. Accessed on February 28, 2020
- National institute of diabetes and digestive and kidney diseases. Vesicoureteral Reflux (VUR).Available at https://www.niddk.nih.gov/health-information/urologic-diseases/hydronephrosis-newborns/vesicoureteral-reflux. Accessed on February 28, 2020
- American Urological Association. Management and screening of primary vesicoureteral reflux in children. Available at. auanet.org/guidelines/vesicoureteral-reflux.Accessed February 28, 2020.
- Indian Society of Pediatric Nephrology. Guidelines Revised Statement on Management of Urinary Tract Infections. Available at. http://medind.nic.in/ibv/t11/i9/ibvt11i9p709.pdf. Accessed February 28, 2020.










 Appointment
Appointment Second Opinion
Second Opinion Call
Call More
More





 correction in children){kind=link}